
A New Diagnosis, A Worm, And An Airway
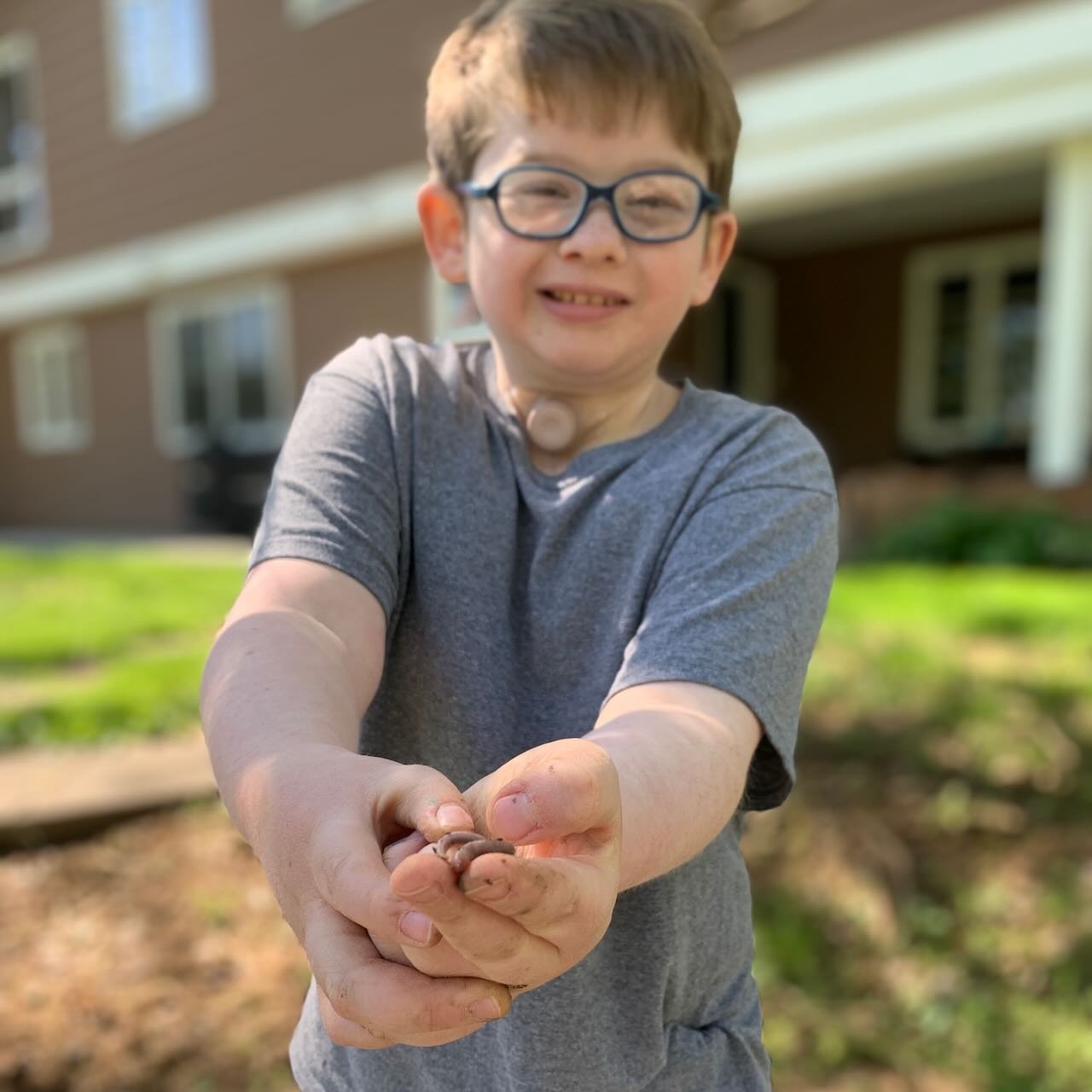
Nathaniel and I traveled to Ohio last week for three appointments at Cincinnati Children’s. This was a follow up from our trip in September when he was diagnosed with Innominate Artery Compression Syndrome. The recent trip was informative. I’ll be sharing the airway surgeon’s suggestions soon. But this morning when Nathaniel held out his dirty hands to show me a worm while we were weeding the flower bed, I saw instantly why this year since the compression syndrome diagnosis has been challenging.
We returned from Cincinnati last fall with instructions to trial living without Nathaniel’s tracheostomy tube. His airway surgery at age four left him with a very stable breathing stoma in his neck. We long ago realized and took advantage of the fact that Nathaniel could go tube free for at least short times without worry that the stoma would close. Over the last few years our routine trach tube changes always included a pause for trach farts where he would look down, expel air between his chest and chin, and then blow harder to make a farting noise. We started the tube free trials immediately in September. By the end of the month, we had fallen into a routine of going tube free all day.
“Going tube free all day” means Nathaniel started living and we started parenting a child with a hole in his neck. Of course, Nathaniel has had a hole in his neck since the day he was born. But I hadn’t considered how I depended on the tracheostomy tube being an initial barrier between the inside of Nathaniel’s body and the world until it was gone. I remember watching him play with Legos in October and wondering if he would, like so many kids who attempt to put small toys up their nose, try to put a Lego in his neck stoma.
This wasn’t our only immediate challenge.
In pediatric tracheostomy world, caregivers are taught and equipped to help manage lung secretions on behalf of the child. We have carried a suction machine with us since Nathaniel was an infant. He wore a barrel shaped heat moisture exchanger (HME) at the end of his tracheostomy tube that did exactly as it sounds - heated and moisturized the air he breathed. It did the job of a nose. In fact professionals, families, and trach kids sometimes call the HME a nose. The secondary blessing of using an HME is that it traps the gunk that children expel from their lungs until the HME is removed for suctioning. When we discontinued using the trach tube in September, we had nothing to attach the pediatric HME to. Nothing to catch the gunk. Our problem, one that we had to mitigate every waking moment since September, was dealing with all the mucus Nathaniel coughs out.
The lack of an HME was also likely creating more mucus. The body’s response to breathing dry air straight into the lungs is to make fluid. September was a long time ago now. It feels like forever since we used pediatric airway management protocols of trach tubes, HMEs, and a suction machine. I can’t remember that way of living well enough to make a comparison between the amount of secretions Nathaniel had with that set up and the amount he has using nothing. But I now know that even a little mucus coughed straight from his neck stoma onto his T-shirt creates a clean up job much messier than using HMEs and suctioning. Guiding a pre-pubescent boy through the process of learning to personally manage bodily fluids isn’t for a faint of heart. This challenge of managing lung secretions with no barrier has created considerable frustration for Nathaniel and caregivers for the last nine months.


Other challenges this year have been equally age specific. Water gun fights. Baths. Rolling off a sled and getting a face and neck full of powdery snow. Hair that sneaks between the cape and neck during a haircut. Stick fights with a nephew. Fingers licked by the dog and then immediately used to wipe away secretions at the stoma. Taking away concerns of germs and others’ illnesses, there have been moments this year when I wanted to yell that it simply does not work for a child to walk around with an exposed hole in his neck. As parents we have simultaneously juggled trying to teach Nathaniel to care for his own airway towards the goal of independence while monitoring dirty hands, environmental concerns, and an open stoma closely to prevent further injury or illness.
But it was different today when he showed me the worm. I could focus on the worm and Nathaniel’s joy. One of our appointments in Cincinnati last week was to meet with an adult medicine doctor who’s team fit Nathaniel and provided us with the products that adults use to protect and humidify neck stomas. We are a handful of days into trialing the new supplies. The hole in Nathaniel’s neck is covered again. Childhood is covered again. The worm, though not necessarily safe in the eleven-year-old’s hands, is safe for Nathaniel.

Therapy Support Found for Pediatric Use of an Eletrolarynx
Nathaniel and I left his Cincinnati Children’s Hospital check up last May with an interesting recommendation from his ENT: look beyond the pediatric community for information and support. I had arrived with questions about Nathaniel’s options for voicing. They shared of another patient with a laryngotracheal separation who learned to use esphageal speech. They also expressed a great deal of hope that given the right support, Nathaniel had a good chance of voicing.

Nathaniel and I left his Cincinnati Children’s Hospital check up last May with an interesting recommendation from his ENT: look beyond the pediatric community for information and support. I had come to the appointment with questions about Nathaniel’s options for voicing. They shared of another patient with a laryngotracheal separation who learned to use esphageal speech. They also expressed a great deal of hope that given the right support, Nathaniel had a good chance of voicing.
Nathaniel and I went to our first Laryngectomy Support Group meeting in June, the very next month. The welcome we received and hope others shared in Nathaniel being able to voice someday brings tears as I try to write. Through out my journey as Nathaniel’s mom, key people have caught my vision for the next possibility for him and then offered ongoing encouragement to pursue the goal. Some Larys (name those with a laryngectomy use to refer to themselves ) from the support group have been added to that short list of names. In December, club members gave Nathaniel an eletrolarynx of his own.
I immediately began networking with group members and their contacts in the local adult medicine and laryngectomy world. Though they work solely with the adult clients, representatives from Atos Medical helped me learn more about options. A speech pathologist for the company spent a lengthy time on the phone one afternoon brainstorming a possible path towards Nathaniel voicing. She outlined steps needed towards the goal. These snippets of information and support motivated me to make the next inquiry and to follow up on the contacts and resources suggested.
The difficulty is the highly specialized field of speech language pathology. Nathaniel needs support in oral motor development, oral motor sound movements that toddlers and young children typically acquire as they develop articulation, and instruction on the use of an eletrolarynx. I found therapists comfortable with some aspects of that puzzle, but until this spring failed to find anyone comfortable charting a path.
In March, Nathaniel spent almost three hours with two clinical professors from a local university’s Department of Communication Sciences and Disorders. One is an expert in articulation, phonological disorders, and childhood apraxia of speech; the other professor’s expertise is in adult acquired communication disorders and specifically with neck and throat cancer patients in the hospital setting. Their time with Nathaniel was watched closely by multiple speech pathology students. The department shared following conclusion in their multiple page report,
“Prognosis is unknown for gaining skill for using electrolarynx. (Nathaniel) has demonstrated some initial success with movements, holding the eletrolarynx himself, producing a few bilabials with the eletrolarynx, and was very cooperative. These are all positive indicators to at least try to train him to able to make oral motor sound movements to eventually use the eletrolarynx."
They are willing to try.
Nathaniel has had three one hour sessions. The clinicians are working on various lip, tongue and jaw movements using verbal cues for each like open mouth, tongue up, tongue down, etc. They are pairing articulatory movements of the mouth for sounds to the hand signals I’ve taught this year for each phoneme and their own voicing. I have cried watching layer after layer of work in Nathaniel’s life, by professionals and myself, provide doors to the next step. We are using some oral motor and sound production apps on the iPad as part of our daily “let’s move our mouths” work at home.
I see changes weekly. Nathaniel is suddenly vocal. That might sound silly being said about a nonverbal child with no use of his vocal cords, but I don’t know how else to explain it. For the first time in his life, he’s doing spit raspberries with his lips. He practiced those through a recent church service. The small child sitting behind us answered; they had great fun going back and forth in full spit raspberry conversation. My brother once said that he noticed Nathaniel moved his mouth when he gestured as if he was trying to speak. I see that almost every time Nathaniel is gesturing or signing now. He is constantly making noises in his cheeks and further back in this throat that I can not duplicate or figure out what he is doing. When we are working on literacy and phoneme work, he is watching my mouth and attempts to copy the movement of my lips and tongue.
With the weekly support, it all seems so logical. The starting point and incremental steps make sense. It strikes me as something I should have figured out and been doing with Nathaniel years ago. But without those critical individuals dreaming and thinking with me and leading me in areas I don’t understand, I couldn’t get momentum. Like the professors have said, Nathaniel ability to voice in the future is unknown. There isn’t research or information in the discipline to give a prognosis on what we are trying to do. I have come to believe that undetermined predictions create Nathaniel’s best opportunities.
What does this mean for our AAC work with Nathaniel’s communication device? Nothing. Esphageal speech or using an eletrolarynx is another form of alternative speech. The university’s clinic is free of charge. We can add these new sessions and continue the weekly sessions with Nathaniel’s speech language pathogist who is working on communication with his device. We are giving him tools. Time and Nathaniel will tell us his preferred method of communication; I suspect it will always be a conglomeration of what is fastest in any given moment. I rarely share video of Nathaniel. But these first steps toward speaking are worth documenting.
Photo above of Nathaniel working with two SLP students in clinic was taken from an observation room and shared with their permission.

Camping with a Tracheostomy
When I googled "camping with a tracheostomy" last week, I mostly found short lists of summer camps that accept medically complex children. A few forums suggested using an RV for traveling and camping experiences with a trach kiddo. We rented a large RV in 2008 and took five children to the Devil's Tower, Badlands, Mount Rushmore, Yellowstone, and the Grand Tetons. I can easily imagine how convenient it would be to "RV camp" with Nathaniel. Except we do not own an RV; we own a tent.

When I googled "camping with a tracheostomy" last week, I mostly found short lists of summer camps that accept medically complex children. A few forums suggested using an RV for traveling and camping experiences with a trach kiddo. We rented a large RV in 2006 and took five children to Devil's Tower, Badlands, Mount Rushmore, Yellowstone, and the Grand Tetons. I can easily imagine how convenient it would be to "RV camp" with Nathaniel. Except we do not own an RV; we own a tent.

The weather has been day after day of too perfect to stay indoors. Nursing coverage is limited just to Friday and Saturday night shifts now, so when our nurse mentioned she might want Saturday night off, we jumped at our chance. We went camping.
There were hot dogs roasted over a fire, chili, s'mores, stars, long talks with friends and family as the fire died out, sleeping bags, cold noses, cold fingers, cold toes, and birds singing too early in the morning. There was also an IV pole, suction machine, heated humidity and compressor, feeding pump, oximeter, and crisp, cool, dry air that threatened creating a mucus plug. But Nathaniel fell asleep in my arms by the fire pit and woke up in a tent, so I can cross "camping" off the bucket list I have in my head for his childhood.
Perhaps next time we'll venture further than the backyard.







Finding Our New Pace
"What if adopting Nathaniel means you can no longer do the things you enjoy doing as a family or individually?" asked the adoption case manager during our staffing interview.
Rich has just finished explaining his and our older boys' involvement in Boy Scouts of America, including the three backpacking trips to Philmont High Adventure Camp. There were fourteen individuals sitting around the table participating in our interview. They had interviewed other couples before us. They were charged with the task of selecting Nathaniel's forever family. Prior to this question, they had described Nathaniel's medical conditions and the many concerns physicians had for his future. The adoption case manager had explained that it was uncertain if Nathaniel would ever walk. "What if he can't hike and go backpacking with you?" the she pushed Rich a bit more. Nathaniel took his first steps nine months later, just a few months after we finalized his adoption.

"What if adopting Nathaniel means you can no longer do the things you enjoy doing as a family or individually?" asked the adoption case manager during our staffing interview.
Rich has just finished explaining his and our older boys' involvement in Boy Scouts of America, including three backpacking trips to Philmont High Adventure Camp. There were fourteen individuals sitting around the table participating in our interview. They had interviewed other couples before us. They were charged with the task of selecting Nathaniel's forever family. Prior to this question, they had described Nathaniel's medical conditions and the many concerns physicians had for his future. The adoption case manager had explained that it was uncertain if Nathaniel would ever walk. "What if he can't hike and go backpacking with you?" she pushed Rich a bit more. Unknown to anyone in the room, Nathaniel would take his first steps nine months later, just a few months after we finalized his adoption.
"I'll carry him," Rich had responded to the adoption worker's question, "we'll find a way to make it work." Conversation about Nathaniel's airway was fairly brief during our adoption interview. Physicians, case managers, foster parents, everyone expected a reconstruction surgery sometime after he was two or three years old. But Nathaniel's airway abnormalities has been and will continue to be the most significant limiting factor for his life and ours. Fourteen months ago we had never left the St. Louis region with Nathaniel. We had roughly two minutes to intervene if Nathaniel's airway was compromised. We stayed on the grid and close to home where first responders could easily get to us. Since airway surgery in February, we have slowly started to envision a different life for Nathaniel. A life that is new to him, but is a return to our family's old life. A life that this weekend did involve carrying Nathaniel. Rich and Josiah are scheduled for a twelve day backpacking trek at Philmont next summer. The scout troop with train with regular local hikes through the year. Rich and I enjoy hiking together too. We recently purchased a Lowepro Fastpack to carry medical supplies and a Thule Urban Glide so Nathaniel can join us. We explored a wonderful, new to us, trail very close to home Saturday morning.




We encountered a handful of other groups the first mile of walking. We were already familiar with the trail conditions. It was peppered with numerous small boulders, tree stumps, and exposed roots. It had steep rocky descents, and muddy, pitted, slippery, stone creek beds. All who crossed our path expressed concern about having the stroller and a small child on such rugged terrain. One man warned of a tree across the path ahead that hikers had to climb through as the branches were too large to move. "Maybe you can find a way around it..." he said. A woman walking alone with her dog mentioned a steep rocky incline ahead. "I don't think a stroller is going to make it; it's pretty rugged." Their comments reminded me of a few friends' comments prior to Nathaniel coming home. "I hear private duty nursing is horrible and very inconsistent. You can't depend on it," one friend had warned. She, like the hikers, were right about the hazards in our path in parenting Nathaniel and on the hike. But the problems faced on either course did not demand we turn back; only that we adjust our expectations of the journey. We went over one branch and under the other when we encountered that downed tree. There was not just one steep rocky incline, but many. I logged twenty-four flights of stairs while on the trail, we carried Nathaniel up all of them. Rich at the front wheel picking our path; I lifted at the handle only able to see the ground as it appeared under the stroller. I learned to place each foot exactly where Rich's foot had just left so I did not slide. Like parenting Nathaniel, we went slow and rested often.
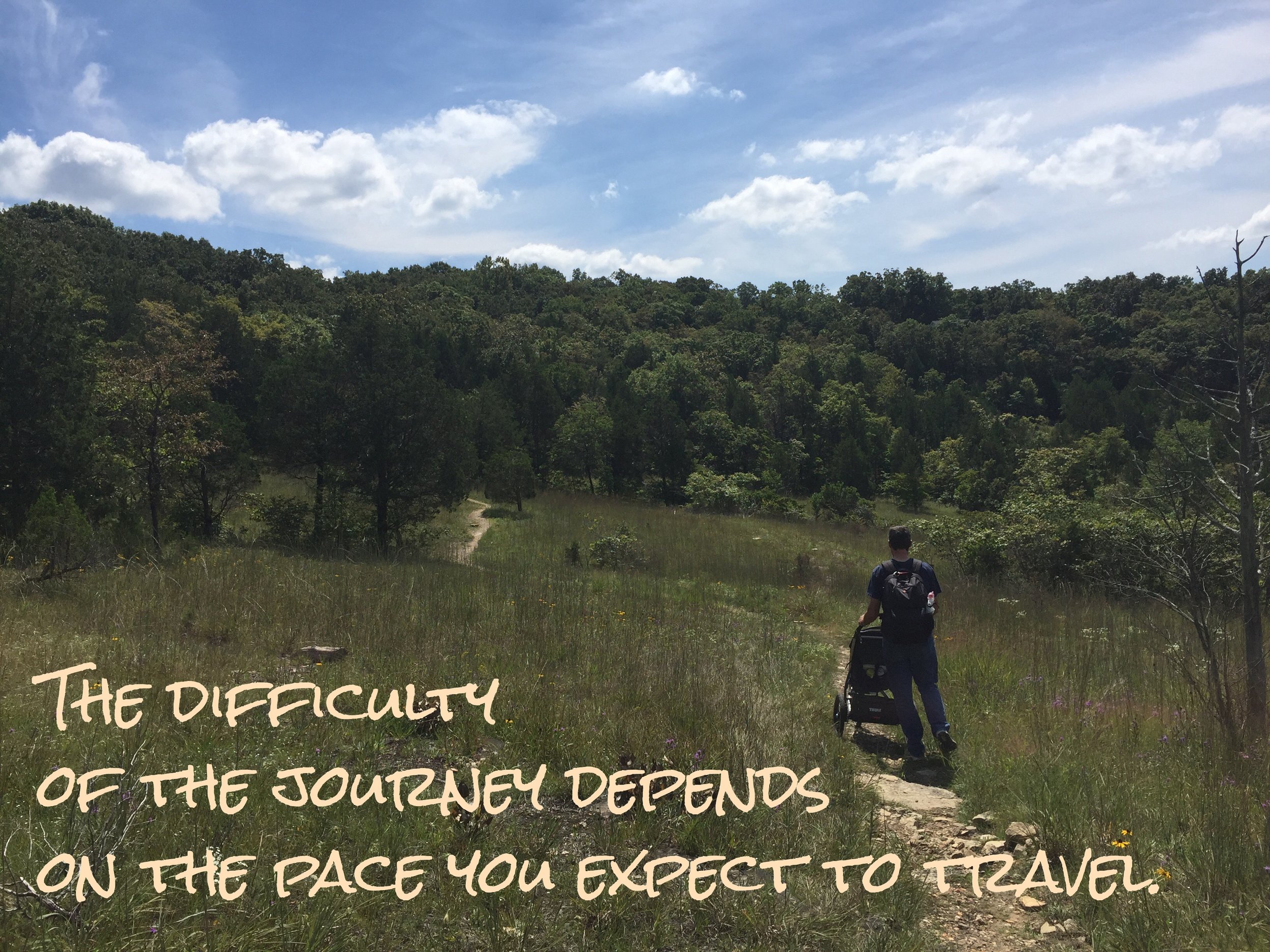
The obstacles along the trail reminded me of the difficulties we have faced in Nathaniel's journey. We were able to navigate some things that seemed big and foreboding, like a large rock, with ease. Some barriers, like a succession of small roots, were more difficult. How tough any one particular roadblock was to us was more determined by the angle we approached, the momentum we had, and how recently we had overcome the last obstacle. At one point in the hike, I came upon a tree root with the front wheel turned slightly to the right. It hit the root and stopped. The left rear tire slid off the trail embankment, pitching the stroller and Nathaniel to the left and requiring enormous force on the ride side of the handle to keep everything aright. The small root should not have required so much energy to overcome, but it did. I suspect this interconnection between the obstacles and our skill at steering through them is why family, friends, therapists, nurses, and others who work intimately with our family are sometimes confused with our ability or inability to manage challenges. We are frequently waylaid by small root sort of problems - too many therapy sessions in a week, a two day hospitalization for a minor virus, a canceled nursing shift - while we sometimes sail past big complications, surgeries, and diagnoses with seeming ease. Our pace is not determined by the individual hurdle only.


A father and son came up from behind as we broke into one of the many glades. They were jogging and quickly overtook us. The father mumbled some comment about "that being burden and slow" pointing to the stroller. We smiled and lightheartedly said, "No, it's not bad." What I wanted to say is that unlike him, we did not start our journey that morning expecting to run. We knew from what we had read about the hike that it would be difficult. We knew it would challenge us. We expected the three miles to take hours. We packed a snack and water. We paused to take photos. We admired countless varieties of mushrooms. We let Nathaniel hike, which was even slower than carrying him in the stroller. We finished, just like the runners, but at our own pace. It is good to reclaim the activities that are at the core of our family culture. It is good to invite Nathaniel into those activities. He, nor his stroller, are a burden, they just helping us find our new pace.

Hello from Cincinnati... Let's Have Cake
had a heavy heart Monday evening when I merged from Interstate 74 south to 275 east. I do not need a map to get to our Cincinnati hotel anymore. I know this city well. We walked into the lobby, and Nathaniel started to cry. He was inconsolable through the check in process and worse when we got to the room. He stood frozen halfway between the bed and the door, held his trach and cried. I had to wipe tears too. Everything about arriving in southern Ohio for another group of appointments felt hard and heavy and sad to both of us. We've done this a lot in the last year. Many of the visits produced physical pain and difficult news. Neither of us wanted to be here.
In the process of settling into the room, Nathaniel's g-button was pulled out. My twelve-year-old niece was in St. Louis last week for her annual "Camp Rankin" visit, and I asked her parents for a second week so she could be my travel companion. She is brave beyond her years. She responded quickly and confidently to instructions and helped to reinsert the button. Nathaniel laying on the floor without his shirt led to tickling and giggles. Ellie is old enough to be a fantastic mother's helper and young enough to be a buddy to Nathaniel.

I had a heavy heart Monday evening when I merged from Interstate 74 south to 275 east. I do not need a map to get to our Cincinnati hotel anymore. I know this city well. We walked into the lobby, and Nathaniel started to cry. He was inconsolable through the check in process and worse when we got to the room. He stood frozen halfway between the bed and the door, held his trach and cried. I had to wipe tears too. Everything about arriving in southern Ohio for another group of appointments felt hard and heavy and sad to both of us. We've done this a lot in the last year. Many of the visits produced physical pain and difficult news. Neither of us wanted to be here.
In the process of settling into the room, Nathaniel's g-button was pulled out. My twelve-year-old niece was in St. Louis last week for her annual "Camp Rankin" visit, and I asked her parents for a second week so she could be my travel companion. She is brave beyond her years. She responded quickly and confidently to instructions. Her help allowed me to address the emergency without difficulty. Nathaniel laying on the floor without his shirt led to tickling and giggles. Ellie is old enough to be a fantastic mother's helper and young enough to be a buddy to Nathaniel.

After the long drive, I failed to realize then that her presence alone was significant. A year ago last week we brought Nathaniel to Cincinnati Children's for the first time for his airway evaluation. We brought three adults. Nathaniel's airway at the time demanded twenty-four hour observation. We didn't drive without an adult in the backseat with him. We had a family member or nurse awake twenty-four hours a day. Upon waking last Friday morning, Nathaniel removed his tracheostomy ties and tube again. The longer window to respond then and the fact that a mature twelve year old can be my travel companion this week are evidence that despite our weary emotions, this last year and the many trips to Cincinnati have yielded positive changes for Nathaniel and all of us.
Ellie, Nathaniel, and I were set to explore the Cincinnati Museum Center today. Her father wanted her to learn about the regional history, and I enjoy the Center's history portion. Win-Win for the adults' interests! Unfortunately that portion of the museum is closed for roof repairs. They redirected us to the Behringer-Crawford Museum in Covington, Kentucky's Devou Park. It was a good redirection. The Outdoor NaturePlay area lifted Nathaniel's and my spirits even more. Ellie collected Ohio River facts and loved the lookout we found at the park.



If you are ever in Covington Kentucky at lunch time, check out Bean Haus Bakery and Cafe. Their iced coffee and cherry smoothie were great. The turkey with smoked gouda sandwich and veggie wrap are highly suggested. The children's games on the book shelf and the dining room to ourselves were a gift. And the gigantic buckeye? No words from this native Ohioan and her niece. By the way, it took Nathaniel precisely one second to realize that throwing Connect Four pieces out the open window near our table was far more fun that playing the game with his cousin.
The nature of our visit to Cincinnati Children's this week is GI issues. Nathaniel gained some freedom to start oral tastings after airway surgery in February, but was placed on the Six Food Elimination diet until more testing and information was gathered. Feeding progress has been slow. Very slow. Nathaniel eats a small number of things okay, but nothing easily. He had a lunch of water, Kix cereal, and his G-tube feed while Ellie and I ate the above delicacies.



We came to Cincinnati wondering if Eosinophilic Esophagitis would be a new diagnosis. It is not. Nathaniel's oral diet restrictions have been lifted. We are now free to offer milk, eggs, wheat, soy, peanuts/treenuts, and shellfish (along with all other foods) one at a time watching for any negative response. There were new diagnoses related to his GI system and a recommendation for a multidisciplinary feeding therapy evaluation. Like other Cincinnati trips, today's news is not the final answer, but provides a directional arrow. Learning to eat for the first time at almost four years old will likely take some work; it is unknown today if and to what degree Nathaniel will depend long term on g-tube feeds. Time and Nathaniel will let us know.
We stopped by my favorite Cincinnati cafe for dinner after the medical appointments. It is my favorite only because I know where it is and what I like there. I have only been to a handful of Cincinnati restaurants. Like hotels, the ones I've been to, I have frequented a lot. Routine is required when life is taxing. The man behind the counter broke into a smile when we walked in. "You're back in town!" he exclaimed. "Did the little one go to the hospital, today?" Yes, I have been there a lot. As Ellie and I ate, I received texts from family and friends celebrating the lifted diet restrictions. They were full of food emojis. It was then I realized that come November, on his fourth birthday, Nathaniel will be allowed to eat birthday cake and ice cream for the first time in his life.
Tears come as I write that sentence. Restrictions lifted leave a gaping hole that is now oddly filled with previously unallowable sorrow. I bought a smash cake when he was one. The photos are adorable, but they don't tell the heart ache of having to wipe his fingers and whisk the cake away as soon as Nathaniel got frosting to his mouth. Photos from birthday two and three don't tell the whole story either - candles he could not blow out set on top of cakes he could not eat. Birthdays are not days to mourn disability, so our family laughed and smiled and accepted this new way for birthdays to be celebrated. We refused to be sad. In the last year Nathaniel has learned to blow bubbles and a whistle through his trachesotomy tube. Perhaps on his fourth birthday, he will blow out his candles. He will probably blow some lung secretions all over the cake in the process, but that's okay. He can have the whole cake to himself this year.
We leave Cincinnati tomorrow. If feeding support can be secured local to home, the plan is to wait a year to return for an annual evaluation with the Areodigestive team. That's good news. It might give Nathaniel time to forget a hotel room's association with pain and require me to need a map again. It gives us lots of time to learn how to eat cake.



I Wish My Child Could Scream... Or at Least Whimper
It was during the second session of developmental language group that I realized another layer of complexity because of Nathaniel's inability to produce any audible noise with this vocal cords.
He can not scream to protect himself from others or get help.

It was during the second meeting of developmental language group that I realized another layer of complexity because of Nathaniel's inability to produce any audible noise with this vocal cords.
He can not scream to protect himself from others or get help.
Nathaniel was playing quietly at the water tub when a playmate decided he wanted the whole side of the three foot by two foot basin to himself. He was playing to Nathaniel's right and moved closer. Closer then became the other boy's left side pressed against Nathaniel's right side. The boy took a step to the left, forcing Nathaniel to do the same to keep his balance. Another step. Another. Each created a slow, but effective nudge moving Nathaniel quietly down the side of the water basin until he suddenly found himself no longer able to reach the water. He stood motionless for a second looking at his new friend. He had no way to vocally protect himself from being treated this way. Nathaniel reached out to touch the boy. He does this a lot with other children, perhaps in absence of being able to connect with them verbally. It was not a push or hard touch, just a reach. The little boy yelled, "Stop it!" high pitched and loud, successfully soliciting a student clinician's attention. "Keep your hands to yourself, Nathaniel," was her response, unaware of what had happened moments before but seeing Nathaniel's still outstretched hand. Nathaniel left the water tub.
One of the challenges facing our family and Nathaniel's therapy team is how to give him the same power and immediacy that a scream, or a cry, or that shouting "HELP," or "NO," or "STOP IT" provides a person with the ability to vocalize. The above scenario, played out in similar ways over trucks or books or everyone's favorite cooking pot in the pretend kitchen, happened over and over at language group this summer. Children are children. They take things, They move into each others' space. They step on toes. When on the receiving side of such injustices, most children protest quickly and loudly. They began learning the moment they were born that creating noise, any kind of noise, brings the help of an adult. Nathaniel did not have that ability. He currently has no quick, loud way to get immediate help.
This realization became even more stark and sad to me when I spent time with my daughter after the birth of her baby. It was time for me to leave and little Blaise was sleeping peacefully in her bassinet beside Bailee's bed. I watched her until the minutes swept past time to go and then walked to the door, Bailee following. She continued to follow me onto the deck of their second floor flat. "You need to stay in the bedroom with her," I said reflecting how I must mother my little one. Bailee scrunched her eyebrows and looked confused. "I'll hear her if she wakes up and cries, Mom. The door is open."
At seven days old, my granddaughter had a communication skill, she had a power, that her Uncle Nathaniel will never have. My granddaughter's cry wakes her mother at night. It will be heard and responded to when she falls off her tricycle or is stuck at the top of a tree. It will be heard and responded to the first time she is pushed down by another child. When stranger-danger makes everyone a villain. When her fingers are stuck in a door. When her heart breaks over a boy. The night before she leaves home for college. I drove the two and a half hours from granddaughter to Nathaniel that morning crying with happiness that my granddaughter's cry will bring her mother from the deck. Crying with sadness that Nathaniel has no cry, no scream, no moan, no whimper.
I very much dislike these layers being pulled away and seeing what is underneath. I dislike how raw and vulnerable it feels. I hate how vulnerable having no scream leaves Nathaniel. Children with disabilities, developmental delays, and special health needs are at higher risk for bullying and abuse, by their peers and adults. The situations and issues I see now - being shifted away from the water table and being misunderstood by the supervising adult - are very minor. But they foreshadow the difficulties we will face in the future with Nathaniel's peers, nurses, teachers, camp counselors, Boy Scout leaders, doctors, youth pastor, and other adults responsible for his well-being. His vulnerability increases others' responsibility. His vulnerability means I could not walk outside leaving the door slightly open trusting I would hear if he woke and needed me..
It was this very issue that caused me to recognize his first alternative communication tool. Nathaniel sleeps with an oximeter on his foot. It reads his oxygen level and heart rate continually and has piercing loud alarm when either go too low or too high. It sounds off the same alarm when the sensor doesn't pick up a reading. Nathaniel found his feet for the first time when he was around a year old. For a week or more, he would wake from his nap, play with his feet, and then explore the oximeter tape and cord. One day, he worked the tape off and the alarm sounded. We started waiting until Nathaniel removed the monitor before responding to him, even though most often we were sitting in the same room. He learned quickly that this was his way to "call us." It was his cry. It gave him power. Nathaniel still removes his oximeter monitor from his foot first thing in the morning, at the end of every nap, and in the middle of the night if he wants adult help.
As he gets older and ventures beyond the nursery and its monitors, we must search for new ways to give Nathaniel a loud, attention-getting sound or noise. The student clinicians at language group were very open to my observations and concerns about the water table; they were equally concerned and suggested we teach him to clap or stomp his foot when he needs immediate adult attention. One of Nathaniel's older brothers designed a small device that fits over his tracheostomy tube that makes a noise when he exhales. We were able to 3D print it and are trialing it often. Nathaniel's therapy team are consulting with other therapists who work with deaf children to learn how they solicit adult attention and help. I am hopeful that we will be able to reduce the size of his alternative communication device and that his fine motor skills will become more refined, both making his talker a more portable and a faster solution. The possibilities are only as endless as our creativity, and I suspect we will find a variety of solutions to fit various and unique environments.
But the bottom line is the bottom line. Nathaniel's airway is shut completely. Permanently. His vocal cords will never move. His voice will always be alternative. His cry for help will always be alternative. His scream will always be alternative. When he needs me in the middle of the night - alternative. When he falls off his tricycle or is stuck at the top of a tree - alternative. When he is pushed down by another child - alternative. When stranger-danger made everyone a villain - alternative. When his fingers are stuck in a door - alternative. When his heart breaks over a girl - alternative. The night before he leaves home for college - alternative. And as hopeful and as creative as I try to be about alternative, I am concerned that alternative might not always solicit the same response as a person crying for help or screaming with human vocal cords. I am concerned alternative will not be loud enough, strong enough, or demanding enough to stop water tub injustices. Or worse injustices. I am concerned that Nathaniel's vulnerability will not always be met with others' increased responsibility. Responsibility to hear alternative. Responsibility to respect alternative. Responsibility to protect and to defend. Responsibility to be the voice for the voiceless. Because admitting my most vulnerable realizations, I must acknowledge that even the best thought out plan for alternative will likely fall short some day, and Nathaniel's dignity, safety, and perhaps very life might be dependent on how those around him react at the moment alternative fails. Nathaniel's dignity, safety, and perhaps very life might be dependent on how those around him see. Dependent on how they hear. Dependent on how they hear my son's silent scream for protection and help.
"I wanted to scream as I stood there, my toes hanging over the edge of the dock. I wanted to let a gut-wrenching howl rip from my disfigured throat toward those clouded skies. I wanted to say every swear word my mother had ever taught me not to say.
I would have settled for a cut-off whimper,
just as long as some kind of sound came from my lips."
What I Didn't Say
Keary Taylor
